
Rare vestibular conditions: Superior semicircular canal dehiscence
What is SSCD?
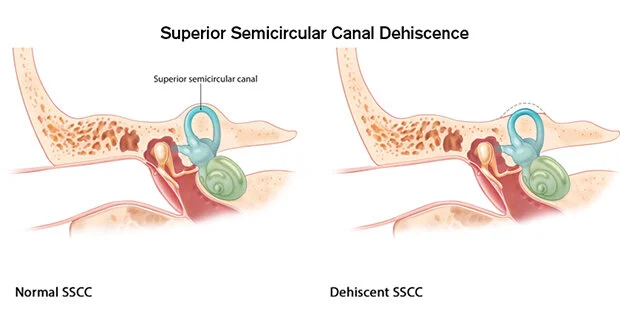
Superior semicircular canal dehiscence syndrome (shortened to SSDC or SSCDS, or also referred to as superior canal dehiscence or SCD) is a rare inner ear condition. SSCD is caused by thin or missing bone in the part of the temporal bone that covers the superior semicircular canal of the vestibular system. This ‘window’ allows for abnormal transmission of pressure between the inner ear and the brain cavity. It is believed that this is congenital (meaning that you are born with it) but there are some cases that seem to arise after head trauma.
What are the symptoms of SSCD syndrome?
The symptoms of SSCD syndrome are often disabling and distressing. Because this condition is rare and many of the symptoms are very uncommon, many people are initially misdiagnosed or told that their symptoms are related to mental health problems.
Some people experience more symptoms related to hearing, and some people experience more symptoms related to dizziness and balance. Symptoms of superior semicircular canal dehiscence syndrome include:
Vertigo, dizziness, or imbalance triggered by sudden loud sounds
Vertigo, dizziness, or imbalance triggered by sneezing, coughing, blowing your nose, or bearing down
Pulsatile tinnitus
Hearing your own voice abnormally loud (autophony)
Hearing your eyes move
Hypersensitivity to sound (hyperacusis)
Bouncing or blurry vision in time with your heartbeat (pulse synchronous oscillopsia)
How do you know if I have SSCD?
The diagnosis is made by asking you questions about your symptoms, doing a thorough clinical exam, and sending you for additional testing.
Clinical signs of SSCD observed during the evaluation include nystagmus triggered by sounds (called the Tullio phenomenon) or by pressure changes (called the Hennebert sign). This is evaluated by looking at your eyes through goggles while using a sound generator, and while using an insufflator bulb or pressing on your tragus (the pointed cartilage at the front of your ear). Tuning fork hearing tests are also used to screen for increased bone conduction.
If SSCD is suspected, the gold standard for assessment is a high resolution CT scan of the temporal bones. The scan will allow your doctor to see if the bone covering over the canal is thinned or missing altogether.
You will also be sent for a hearing test, since in SSCD the audiogram usually shows a low frequency conductive hearing loss. Vestibular function tests are recommended including video nystagmography (VNG), vestibular evoked myogenic potentials (VEMPs, which usually show lowered thresholds in SSCD), and electrocochleography (ECOG, which usually show elevated SP/AP ratios in SSCD).
Treatment for SSCD
The primary treatment for SSCD is surgery. Canal occlusion surgery uses your own tissue to plug the affected superior semicircular canal. This procedure is quite effective in relieving symptoms.
Vestibular rehab for SSCD
A qualified vestibular rehabilitation physiotherapist can determine if you might have symptoms due to SSCD from a thorough interview and clinical exam. If your physiotherapist suspects this condition, they will work with your family doctor to get you a referral to an otolaryngologist (ENT).
Aside from recognizing it as a rare but possible cause of vertigo, the primary role of vestibular rehab physiotherapy in SSCD comes after canal occlusion surgery. As canal occlusion surgery de-functions the superior canal, post-operative gaze stability exercises and balance exercises will help facilitate the compensation process and help you feel better faster. In our clinic at Toronto General Hospital, our physiotherapists work closely with the ENT surgeons. We usually see patients within a few days post-operatively to start vestibular exercises, and communicate directly with the surgeon regarding your progress in rehab. The prognosis with rehab is excellent - patients are usually expected to return to normal activities without symptoms.
-
Suzuki M, Ota Y, Takanami T, Yoshino R, Masuda H. Superior canal dehiscence syndrome: A review. Auris Nasus Larynx. 2024;51(1):113-119. [link]
Ward BK, Van De Berg R, Van Rompaey V, et al. Superior semicircular canal dehiscence syndrome: Diagnostic criteria consensus document of the committee for the classification of vestibular disorders of the Bárány Society. VES. 2021;31(3):131-141. [link]
Öhman J, Forssén A, Sörlin A, Tano K. Patients’ experiences of living with superior canal dehiscence syndrome. International Journal of Audiology. 2018;57(11):825-830. [link]